Rebecca Barnes’s Poster
Why Do Clinicians Struggle to Establish a Good Alliance with High-Risk Patients? An Investigation of Clinicians’ Intrapersonal Factors
by Rebecca Barnes1, Alexis Berman2, Jimmy Pengyu Chen3,4, & Sarah Bloch-Elkouby2,4
1 City College of New York
2 Ferkauf Graduate School of Psychology, Yeshiva University
3 Teachers College, Columbia University in the City of New York
4 Icahn School of Medicine at Mount Sinai in New York City
Background:
Recent literature has shown that clinicians struggle to establish an effective alliance with patients at high risk for suicide, and that clinicians often experience negative emotional responses towards these patients (Bloch-Elkouby & Barzilay, 2021; Newkirk & Galynker, 2022; Regehr et al., 2015).
To date, the literature examining the possible mechanisms responsible for these phenomena remains very sparse. In light of the critical importance of the alliance when working with high-risk patients, the value of shedding light on clinicians’ intrapersonal processes that may contribute to a poor alliance cannot be overstated (Michaud et al., 2021; Soulié et al., 2021).
Hypotheses:
- The higher the risk level assessed by clinicians, the lower their experience of the alliance.
- This relationship (the alliance) will be mediated by clinicians’ negative emotions towards their high-risk patient.
Method:
Eighty-six clinicians conducted an initial interview with a virtual (i.e. photorealistic AI-powered) White male adolescent patient.
Immediately after the interview, clinicians were asked to assess the level of suicide risk of the patient using the Clinician Prediction Scale (CPS, Nock, 2010), followed by a self-report measure about their emotional response to the patient (TRQ-SF; Barzilay et al, 2018) and by the clinician-rated version of the Rupture Resolution Rating System (3RS, Eubanks et al., 2020).
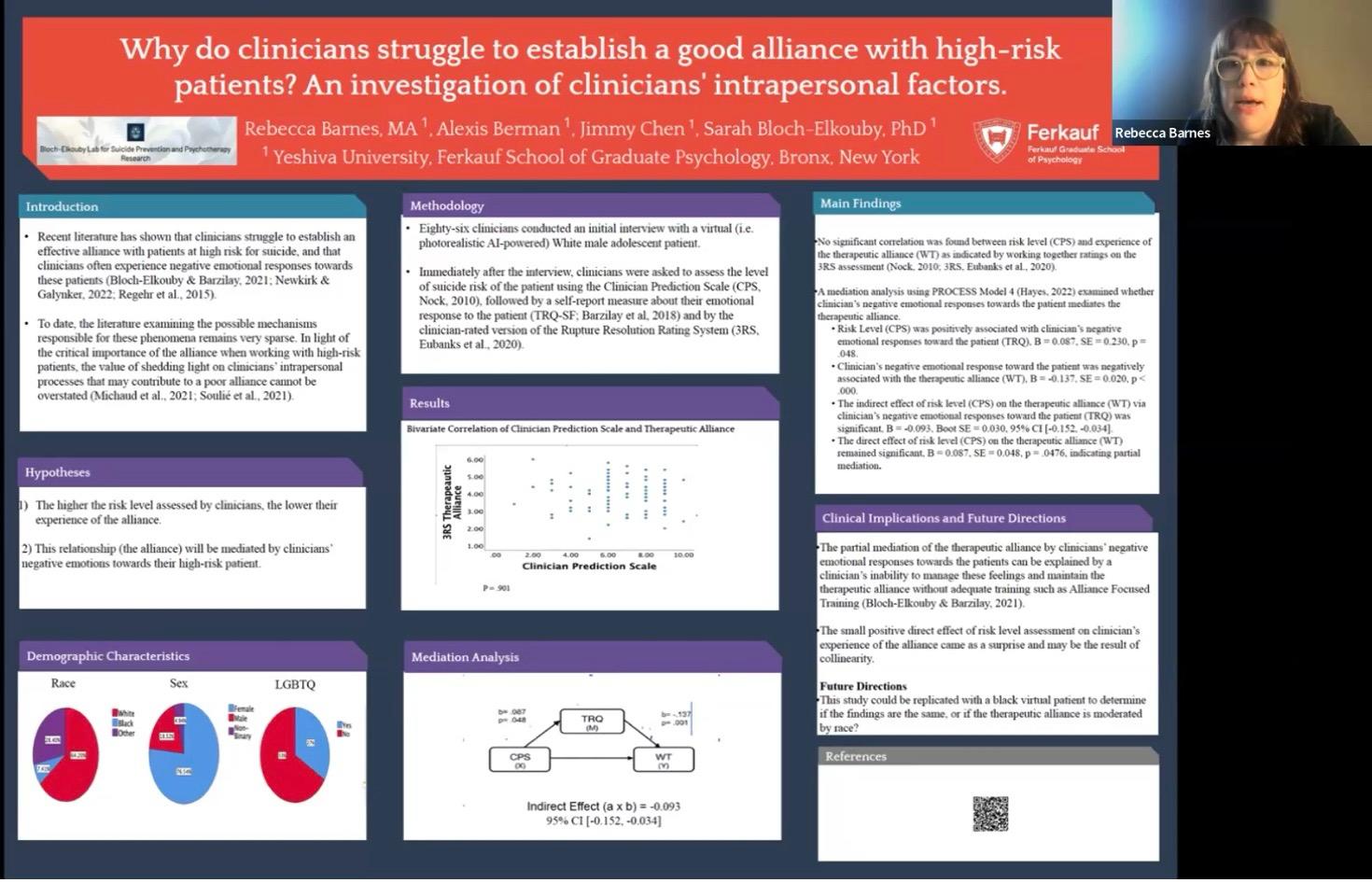
Results:
No significant correlation was found between risk level (CPS) and experience of the therapeutic alliance (WT) as indicated by working together ratings on the 3RS assessment (Nock, 2010; 3RS, Eubanks et al., 2020).
A mediation analysis using PROCESS Model 4 (Hayes, 2022) examined whether clinician’s negative emotional responses towards the patient mediates the therapeutic alliance.
- Risk Level (CPS) was positively associated with clinician’s negative emotional responses toward the patient (TRQ), B = 0.087, SE = 0.230, p = .048.
- Clinician’s negative emotional response toward the patient was negatively associated with the therapeutic alliance (WT), B = -0.137, SE = 0.020, p < .000.
- The indirect effect of risk level (CPS) on the therapeutic alliance (WT) via clinician’s negative emotional responses toward the patient (TRQ) was significant, B = -0.093, Boot SE = 0.030, 95% CI [-0.152, -0.034].
- The direct effect of risk level (CPS) on the therapeutic alliance (WT) remained significant, B = 0.087, SE = 0.048, p = .0476, indicating partial mediation.
Conclusion:
The partial mediation of the therapeutic alliance by clinicians’ negative emotional responses towards the patients can be explained by a clinician’s inability to manage these feelings and maintain the therapeutic alliance without adequate training such as Alliance Focused Training (Bloch-Elkouby & Barzilay, 2021).
The small positive direct effect of risk level assessment on clinician’s experience of the alliance came as a surprise and may be the result of collinearity.
Future Directions This study could be replicated with a black virtual patient to determine if the findings are the same, or if the therapeutic alliance is moderated by race?
References:
Barzilay, S., Yaseen, Z. S., Hawes, M., Gorman, B., Altman, R., Foster, A., Apter, A., Rosenfield, P., & Galynker, I. (2018). Emotional Responses to Suicidal Patients: Factor Structure, Construct, and Predictive Validity of the Therapist Response Questionnaire-Suicide Form. Frontiers in Psychiatry, 9, 104. https://doi.org/10.3389/fpsyt.2018.00104
Bloch-Elkouby, S., & Barzilay, S. (2021). Alliance-focused safety planning and suicide risk management. Psychotherapy, 59(2), 157-162. https://doi.org/10.1037/pst0000416
Eubanks, C. F., Lubitz, J., Muran, J. C., & Safran, J. D. (2018). Rupture Resolution Rating System (3RS): Development and validation. Psychotherapy Research, 29(3), 306–319. https://doi.org/10.1080/10503307.2018.1552034
Hayes, A. F. (2022). PROCESS Macro for SPSS and SAS. The PROCESS Macro for SPSS, SAS, and R. https://www.processmacro.org/index.html
Huggett, C., Gooding, P., Haddock, G., Quigley, J., & Pratt, D. (2022). The relationship between the therapeutic alliance in psychotherapy and suicidal experiences: A systematic review. Clinical Psychology & Psychotherapy, 29(4), 1203–1235. https://doi.org/10.1002/cpp.2726
Michaud, L., Greenway, K. T., Corbeil, S., Bourquin, C., & Richard-Devantoy, S. (2021). Countertransference towards suicidal patients: a systematic review. Current Psychology, 42, 416-430. https://doi.org/10.1007/s12144-021-01424-0
Newkirk, S., & Igor Galynker. (2023). Clinician Emotional Response to Patients at Risk of Suicide: A Review of the Extant Literature. In M. Pompili (ed), Suicide risk assessment and prevention (pp. 167-181). Springer, Cham. https://doi.org/10.1007/978-3-030-42003-1_86
Nock, M. K., Park, J. M., Finn, C. T., Deliberto, T. L., Dour, H. J., & Banaji, M. R. (2010). Measuring the suicidal mind: Implicit cognition predicts suicidal behavior. Psychological Science, 21(4), 511–517. https://doi.org/10.1177/0956797610364762
Regehr, C., LeBlanc, V. R., Bogo, M., Paterson, J., & Birze, A. (2015). Suicide risk assessments: Examining influences on clinicians’ professional judgment. American Journal of Orthopsychiatry, 85(4), 295–301. https://doi.org/10.1037/ort0000075
Soulié, T., Jenkin, G., Collings, S., & Bell, E. (2023). Relationship between clinicians’ inclination toward patients at risk for suicide (PRS) and self-reported countertransference. Archives of Suicide Research, 27(1), 148-155. https://doi.org/10.1080/13811118.2021.1972883